

Did you know that the Environmental Protection Agency is facing a federal lawsuit that questions the longstanding practice of water fluoridation? Many are unaware of this news. Yet, we may soon see an end to this practice as the stakes are more than just cavities—it’s the neurological health of our children.
Silently flying under the radar the landmark TSCA trial is finally entering into its final hearing. A coalition of nonprofit organizations are suing the EPA for failure to protect the public from water fluoridation.1,2 It’s astonishing and somewhat concerning that a nonprofit organization is the one leading the awareness of these scientific changes.
The dental community finds itself in a precarious position. As a concerned dentist, I’m breaking my silence on this topic to speak on my beliefs concerning fluoride and its effect on our overall health. I want to provide an evidence-based, yet balanced, perspective to this controversial topic.
The plaintiffs have provided substantial evidence that exposure to fluoridated chemicals are neurotoxic – particularly to pregnant women and early infancy. Recent prospective birth cohort studies looking at prenatal exposure to water fluoride at concentrations similar to the US ( 0.7-1.2mg/l) found a significant reduction in children’s IQ scores. There were significant and large adverse effects on developing brains on par with established neurotoxins like Lead, Mercury, and Arsenic. They found lower IQ scores for boys around 5-9 point reductions.3,4
Esteemed epidemiologists and toxicologists like Dr. Howard Hu, Phillipe Grandjean, and Lanphear have been called as expert witnesses against the EPA. These experts have helped establish other environmental neurotoxins like lead, mercury, and arsenic. The likelihood of these scientists becoming renegades is low considering the body of evidence that has been presented in the court case. Some of the EPAs own scientists have even been deposed against the EPA. 1,2
So, is it possible to have too much fluoride? Yes! This has been confirmed by the National Toxicology Program who recently released a 6-year report on the state of the current science concerning fluoride exposure and neurodevelopmental and cognitive health effects. The NTP is a branch of the US Department of Health and Human Services tasked with evaluating and establishing safety levels for exposure to environmental toxins and carcinogens. This report included a monogram and a meta-analysis. The meta-analysis found that 52 of 55 highly consistent studies found lower IQ with higher fluoride exposures. Of the 19 studies rated higher quality, they found that 18 studies consistently found an IQ-lowering effect in children with prenatal fluoride exposure.5 In another study after pooling the data they found neurotoxic effects at 0.2mg/L, which is below what we typically fluoridate our municipal water systems in the US.6 Additionally previous estimates for the overall prevalence of dental fluorosis have been underestimated. Dental fluorosis is a condition that causes changes in the appearance of tooth enamel when there is overexposure. New NHANES data show an overall weighted occurrence of 87.3% of children and adolescents exhibited some degree of fluorosis in the US.7,8

There’s no doubt that fluoride reduces tooth decay, but at what cost? In light of these findings, I have re-evaluated my own approach to fluoride. That being said I still believe that the dose makes the poison. The problem is that we have been inundated with fluoride due to systemic exposure through water fluoridation as a society. Based on my own thorough evaluation of the studies I firmly advocate for the removal of fluoride from municipal water systems. The emerging evidence has led me to conclude that its presence in drinking water poses unacceptable risks to public health, particularly for vulnerable populations such as pregnant women and their developing babies.
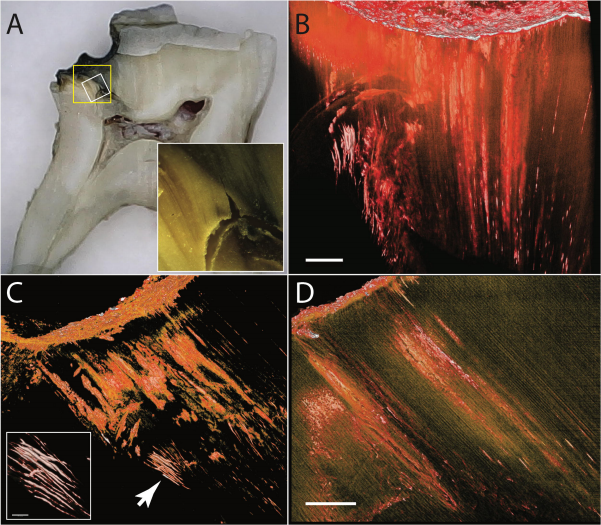
In my clinic, I have been applying fluoride judiciously. The science of the topical benefits is well understood to assist with creating a more resistant tooth structure to tooth decay along with remineralization of tooth decay. I have personally seen the benefits of controlled topical application of fluoride in the form of silver diamine fluoride (SDF) & sodium fluoride to arrest early tooth decay in my own mouth. When faced with the decision to irreversibly remove natural tooth structure with a filling, I decided that a conservative minimally invasive approach was the better route. Below is a picture of how SDF arrested tooth decay allowing for this pediatric patient's primary tooth to exfoliate naturally without the tooth becoming infected.9 They have also performed studies showing no systemic toxic side effects after application of SDF.10
I still see this application of topical fluoride as a medication that can be helpful. Another example of fluoride application in dentistry that I advocate for is the use of glass ionomer cements. Composite resin fillings have a high recurrence rate of tooth decay underneath them. For pediatric patients composites are not great long-term options. In this case, Glass Ionmer fillings are bioactive and assist in healing the tooth by releasing fluoride and laying down hydroxyapatite.11 As more research and material development continues, I’m sure that we’ll rely on fluoride less each year, but I firmly believe that glass ionmer materials are some of the best options for pediatric patients.
In the realm of dental health, the debate over fluoride's efficacy and safety has long been a topic of contention. On both sides of the debate, the heart of this hot topic lies within the pressing issue of caries, or tooth decay. This disease remains a major issue in the United States. Recent statistics from the Centers for Disease Control and Prevention (CDC) reveal a disconcerting reality: over half (52%) of children 6 to 8 years of age have had a cavity in their primary (baby) teeth. Among adolescents aged 12 to 19, more than half (57%) have had a cavity in their permanent teeth. Among adults aged 20 and older, about 90% have had at least one cavity. Despite advancements in dental care, caries persist as one of the most common chronic diseases, affecting individuals of all ages and socioeconomic backgrounds.12
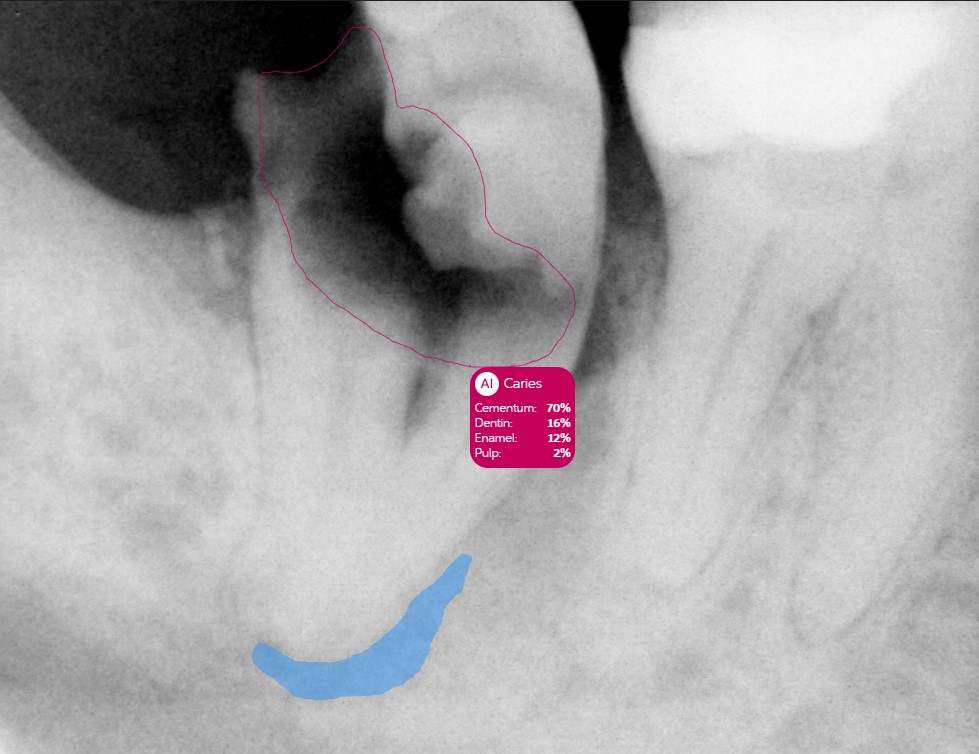
For people who frequently eat highly refined carb diets and drink plenty of acidic beverages, the bacteria in the mouth ferment these sugars and create acid. This acid starts to erode and break down the tooth. The tooth consists of the outer layer called the enamel (white), the dentin layer (green), and the pulp (magenta).
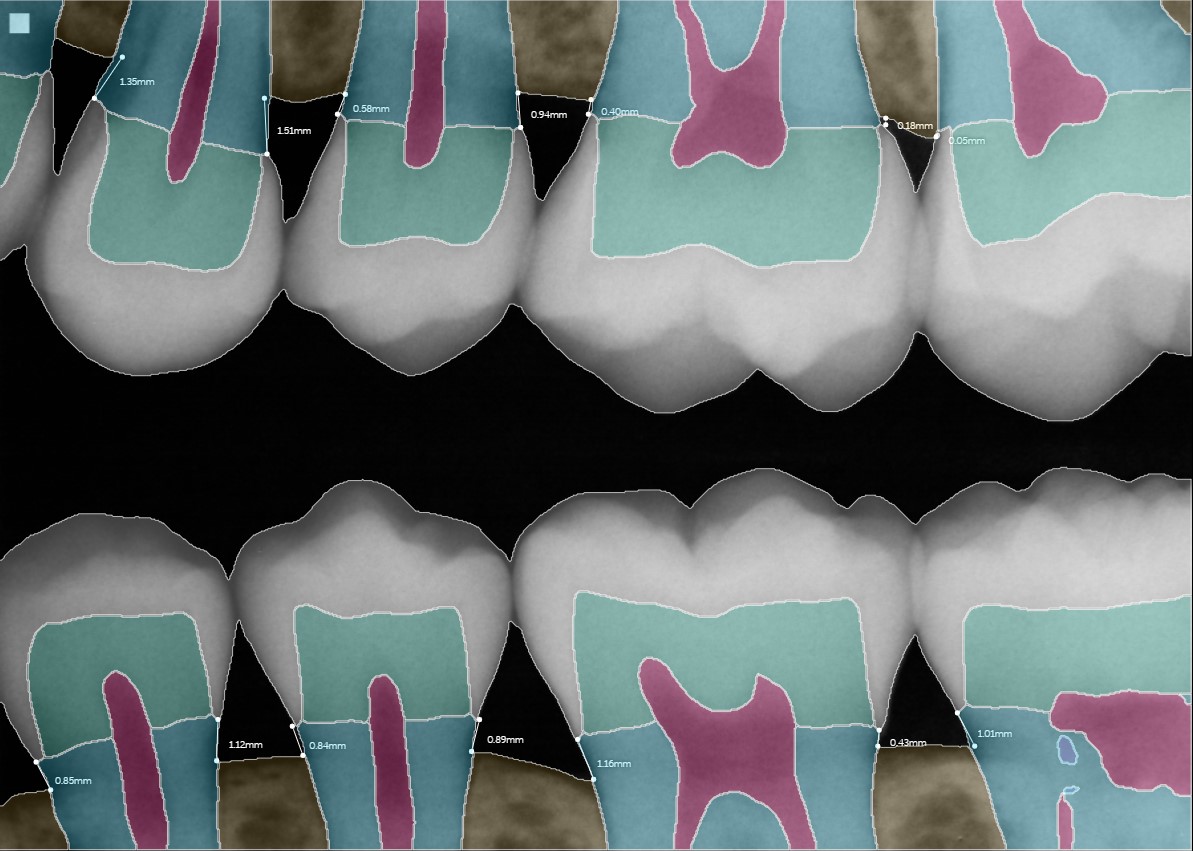
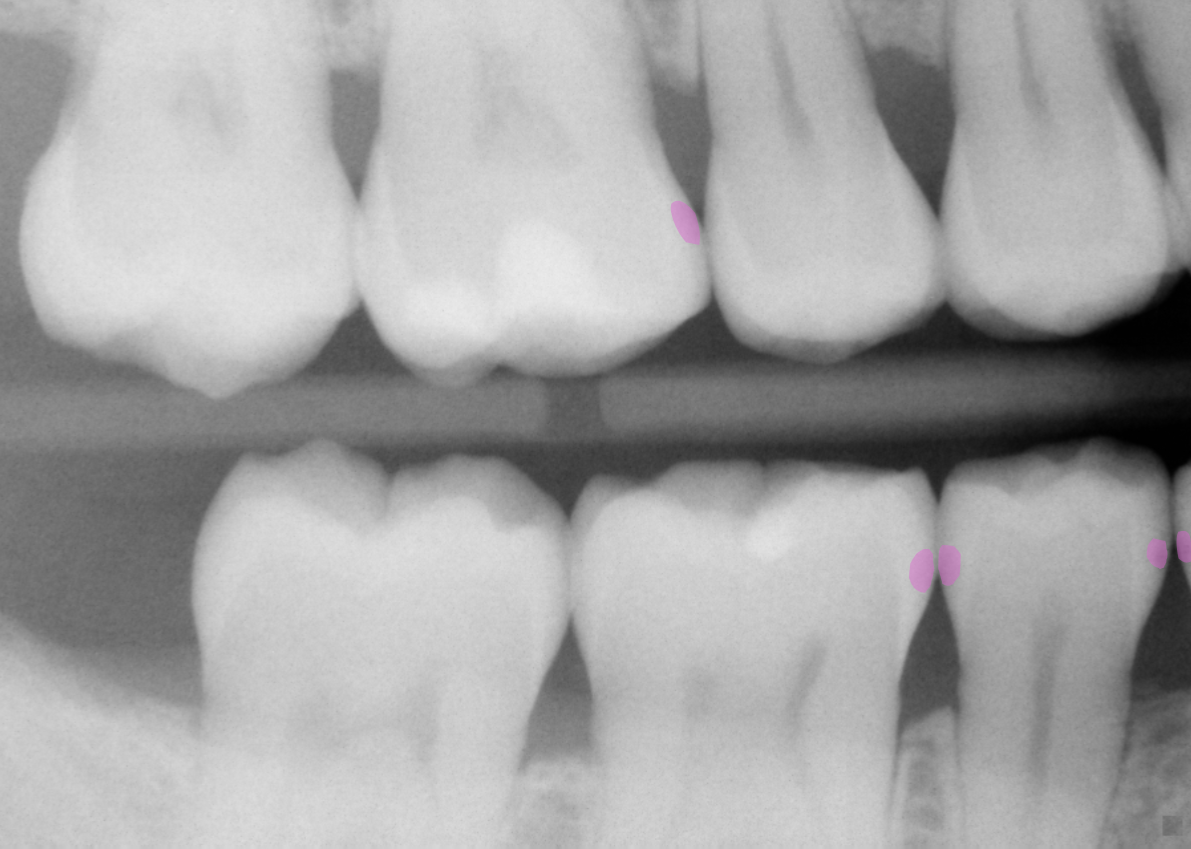
When a cavity is small, like in the x-rays in the figure below, the teeth have the capacity to remineralize.
Cavities confined to the enamel are where fluoride can be used to arrest caries, avoiding the need for drill and fill dentistry. Proper nutrition providing fat soluble vitamins and minerals for the saliva can also assist at this stage.
As bacteria continue to ferment sugars into acid, the cavity will progress into the inner dentin layer. The dentin is less mineralized compared to the enamel layer and more prone to fast progression of the decay.
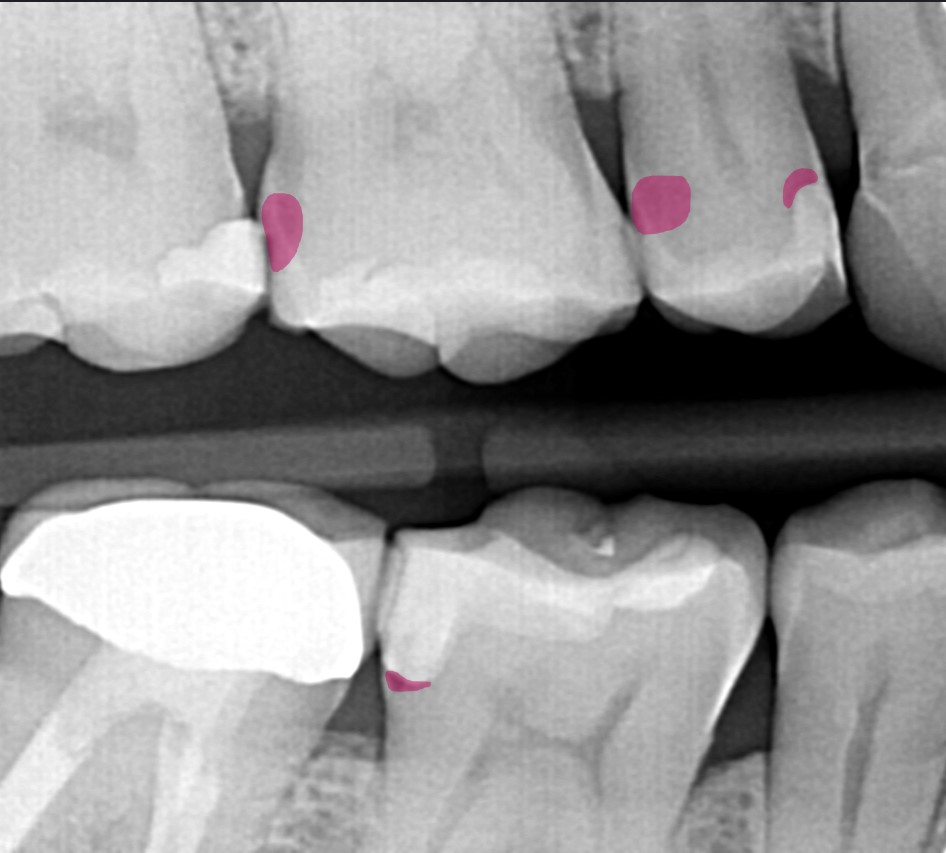
If left untreated the tooth will become infected and lead to a painful abscess. An abscess (a severe infection) can spread to other parts of the body and have serious, and in rare cases fatal, results.
There are major consequences to poor dental health. In the ongoing debate surrounding fluoride, it's important to recognize that both sides share a common goal: promoting optimal dental health while minimizing potential risks. Proponents of fluoride argue that it plays a crucial role in preventing tooth decay by strengthening enamel and reducing the risk of cavities, particularly in communities where access to dental care may be limited. On the other hand, critics raise valid concerns about potential adverse effects, such as dental fluorosis and neurotoxicity, especially with prolonged exposure or in vulnerable populations.
However, amidst this polarization, there is common ground in the acknowledgment of the importance of dental hygiene practices, regular dental check-ups, and access to oral health education. By fostering dialogue and collaboration between proponents and critics, we can strive towards a balanced approach that prioritizes both oral health and safety for all individuals.
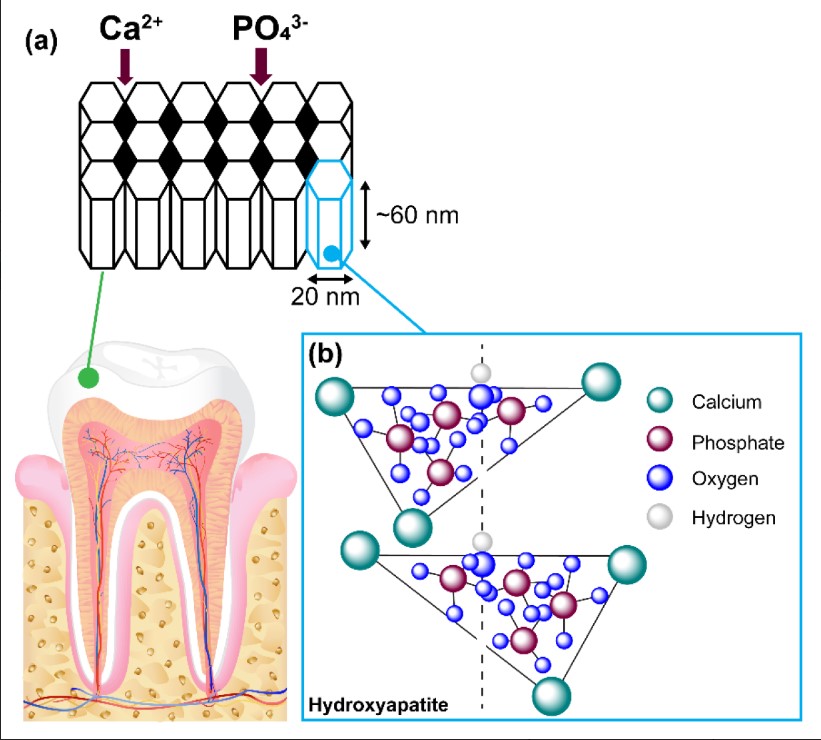
Moving forward, my dental office is committed to offering a comprehensive range of alternatives to traditional fluoride treatments, catering to the diverse needs and preferences of our patients. In addition to conventional fluoride applications, we now provide biomimetic options such as the application of hydroxyapatite varnish and hydroxyapatite toothpastes. This substance is the same building block that makes up our bones and the enamel of our teeth. Hydroxyapatite has compelling evidence for enamel regeneration and prevention of tooth decay without the potential risks associated with fluoride.13,14,15
Additionally, we are excited to implement self-assembling peptide treatments that mimic the body's natural enamel-building process. Both of these cutting-edge technology have shown great potential in promoting enamel regeneration and combating dental caries.16,17
Furthermore, we recognize the importance of selectively using topical applications of fluoride, tailored to individual patient circumstances. For patients with thyroid issues or those who are pregnant, these alternative options may offer safer alternatives, as concerns have been raised regarding the potential impact of fluoride on thyroid function and fetal development in this court case.
It turns out that the best defense against tooth decay might not be in the water we drink but in the wholesome foods we choose to eat. We emphasize the crucial role of nutrition in oral health providing guidance on dietary choices that support strong teeth and gums. By offering a diverse array of alternatives and personalized recommendations, we aim to empower our patients to make informed decisions about their oral health, ensuring optimal outcomes for all.
Fluoride’s benefits are best found in topical form and applied in the hands of a trained professional. That said, water fluoridation or topical applications have never resolved the true issue of tooth decay. This is not a disease caused by fluoride deficiency but by nutritional deficiency and salivary composition changes contributing to microbiome imbalances. I’m excited to see where the field will head as it’s becoming increasingly apparent that what happens in the mouth is not isolated from the rest of the body, but deeply connected to overall health and well-being. I welcome the change!
References:
- Gravitz L. The fluoride wars rage on. Nature. Published online October 27, 2021. doi:10.1038/d41586-021-02924-6
- Fluoride Action Network. Fluoride On Trial: Federal Trial on the Neurotoxicity of Water Fluoridation Resumes. Fluoride Action Network. Accessed February 19, 2024. https://fluoridealert.org/articles/fluoride-on-trial/
- Bashash M, Thomas D, Hu H, et al. Prenatal Fluoride Exposure and Cognitive Outcomes in Children at 4 and 6-12 Years of Age in Mexico. Environ Health Perspect. 2017;125(9):097017. Published 2017 Sep 19. doi:10.1289/EHP655
- Green R, Lanphear B, Hornung R, et al. Association Between Maternal Fluoride Exposure During Pregnancy and IQ Scores in Offspring in Canada. JAMA Pediatr. 2019;173(10):940-948. doi:10.1001/jamapediatrics.2019.1729
- National Toxicology Program. Fluoride: Systematic Literature Review on Developmental Neurotoxicity. National Toxicology Program. [Accessed February 17, 2024]. Available from: https://ntp.niehs.nih.gov/whatwestudy/assessments/noncancer/ongoing/fluoride.
- Grandjean P, Hu H, Till C, et al. A Benchmark Dose Analysis for Maternal Pregnancy Urine-Fluoride and IQ in Children. Risk Anal. 2022;42(3):439-449. doi:10.1111/risa.13767
- Hung M, Hon ES, Mohajeri A, Moparthi H, Vu T, Jeon J, Lipsky MS. A National Study Exploring the Association Between Fluoride Levels and Dental Fluorosis. JAMA Netw Open. 2023 Jun 1;6(6):e2318406. doi: 10.1001/jamanetworkopen.2023.18406. PMID: 37351888; PMCID: PMC10290240.
- Centers for Disease Control and Prevention. Dental Fluorosis. https://www.cdc.gov/fluoridation/faqs/dental_fluorosis/index.htm. Accessed [19 Feb. 2024]
- Seto J, Horst JA, Parkinson DY, Frachella JC, DeRisi JL. Enhanced Tooth Structure Via Silver Microwires Following Treatment with 38 Percent Silver Diamine Fluoride [published correction appears in Pediatr Dent. 2020 Jul 15;42(4):248]. Pediatr Dent. 2020;42(3):226-231.
- Duangthip D, Fung MHT, Wong MCM, Chu CH, Lo ECM. Adverse Effects of Silver Diamine Fluoride Treatment among Preschool Children. J Dent Res. 2018;97(4):395-401. doi:10.1177/0022034517746678
- Gurgan S, Kutuk ZB, Ergin E, Oztas SS, Cakir FY. Clinical performance of a glass ionomer restorative system: a 6-year evaluation. Clin Oral Investig. 2017;21(7):2335-2343. doi:10.1007/s00784-016-2028-4
- CDC. (2024). FastStats - Cavities (Dental Caries) [Online]. Retrieved from https://www.cdc.gov/oralhealth/fast-facts/cavities/index.html#print
- Dissanayake SSM, Ekambaram M, Li KC, Harris PWR, Brimble MA. Identification of Key Functional Motifs of Native Amelogenin Protein for Dental Enamel Remineralisation. Molecules. 2020; 25(18):4214. https://doi.org/10.3390/molecules25184214
- Burhenne M. Current Research on Hydroxyapatite Toothpaste Efficacy and Safety. Ask the Dentist. https://askthedentist.com/hydroxyapatite-studies/. Accessed [19 Feb. 2024].
- Amaechi BT, AbdulAzees PA, Okoye LO, Meyer F, Enax J. Comparison of hydroxyapatite and fluoride oral care gels for remineralization of initial caries: a pH-cycling study. BDJ Open. 2020;6:9. Published 2020 Jul 22. doi:10.1038/s41405-020-0037-5
- Keeper JH, Kibbe LJ, Thakkar-Samtani M, et al. Systematic review and meta-analysis on the effect of self-assembling peptide P11-4 on arrest, cavitation, and progression of initial caries lesions. J Am Dent Assoc. 2023;154(7):580-591.e11. doi:10.1016/j.adaj.2023.03.014
- Godenzi D, Bommer C, Heinzel-Gutenbrunner M, Horst Keeper J, Peters K. Remineralizing potential of the biomimetic P11-4 self-assembling peptide on noncavitated caries lesions: A retrospective cohort study evaluating semistandardized before-and-after radiographs. J Am Dent Assoc. 2023;154(10):885-896.e9. doi:10.1016/j.adaj.2023.07.009



